
In healthcare, results really matter
Understanding why certain treatments and procedures work better on some patients and not so well on others is the key to delivering more personalized care and ultimately achieving better results for all stakeholders in the care process. The treatment of musculoskeletal conditions, including osteoarthritis in particular, is associated with high resource utilization and substantial variability in choice of treatment and resulting outcomes. For example, the prevalence of osteoarthritis and associated joint replacement surgeries are both on the rise. It’s estimated that 30 million Americans have osteoarthritis today and that more than 1 million total joint arthroplasties (TJA) are performed each year – with 4 million annually by 20301. The same is true for other musculoskeletal treatments including spine procedures. Payers are taking notice and are increasingly exploring value-based care contracts. Patients are becoming more engaged and demanding more evidence. Clinicians are working to deliver better care at lower costs, such as through reducing variability. However, simply cutting costs is not a sustainable strategy. Orthopedic and spine surgeons need new tools. Through artificial intelligence (AI) and predictive analytics, clinicians and patients can gain more personalized and precise estimates of future benefits, risks and costs and make better decisions earlier in the treatment process.
The Basics of AI and Predictive Modeling
AI refers to a set of technologies based on algorithms that enable computer systems to learn from patterns using very large data sets. AI includes machine learning, deep learning, and natural language processing. The latter refers to the ability of the systems, for some purposes, to use free form text, such as clinician notes. A particularly useful application of AI in healthcare is in the generation of predictive models. Using existing clinical data, for example from electronic medical records, and machine learning technologies, high-performing predictive models can be deployed that can identify which patients are most at risk, what outcomes may be expected, and what individual risk factors may be modified to improve expected outcomes. For example, we have developed a machine learning based model, the OM1 Medical Burden Index™ (OMBI™), that measures the aggregate disease burden of the patient and is a very strong predictor of many outcomes, including complications and future costs. Use of AI and predictive models is no longer restricted to academic centers. Streamlined implementation and simple user interfaces enable high powered information to be delivered to where it is most likely to effect change, from community hospitals to physician offices.
Shifting to Value-Based Care
Predictive models are useful when considering value-based care requirements, such as bundled payment programs. For example, within the past several years, the Centers for Medicare and Medicaid Services (CMS) and commercial payers have implemented bundled payment programs, such as for hip and knee replacements. Goals of the hip and knee bundled payment programs include holding hospitals responsible for the quality and total costs of a hip or knee replacement and incentivizing hospitals to avoid expensive and harmful events. Under these models, providers assume greater reward for lower costs and potentially higher financial risk for excessive costs of patient care during the bundle period.2 Both the rewards and risks make it critical for organizations to be able to identify high risk patients and to proactively take actions to avoid high cost events where possible. In hip and knee replacements, non-routine discharges, complications, and readmissions account for $3,309 in excess costs on average for every case performed or $3 billion annually in the U.S.3 Avoiding these complications even for a subset of patients can result in significant costs savings and improved outcomes for patients alike. While the initial bundle payment programs, including in orthopedics, met with mixed reactions, many organizations learned how to be successful under these programs. In fact, the slimmed down BPCI Advanced program from CMS has been surprisingly popular, enrolling more than 1000 entities.
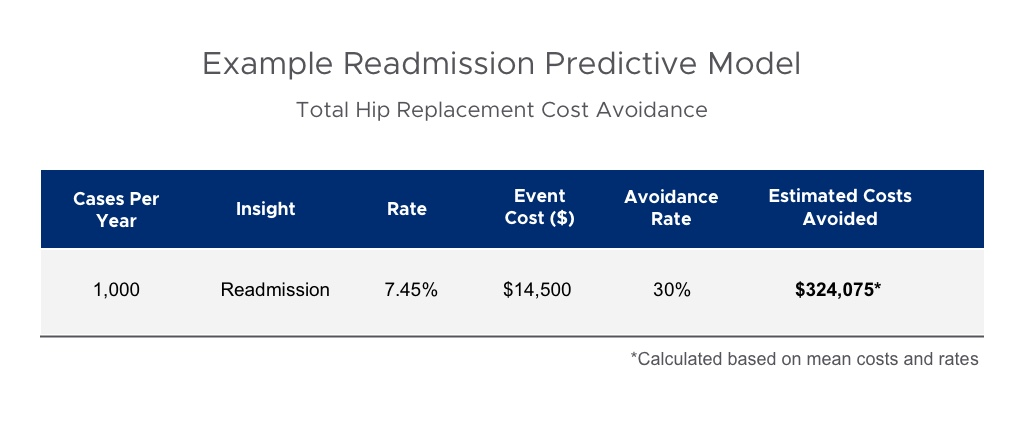
The role of AI for all programs in value-based care is growing. For example, hip and knee predictive models can accurately identify patients at highest risk for high cost and serious complications such as mortality, infection, readmission, reoperation and so forth. More importantly, the models identify actions that can be taken to reduce risk. For example, deferring timing of surgery to better optimize a patient and thereby avoiding an adverse event or readmission can result in significant savings in real dollars. The average readmission cost for a total hip replacement is $14,500 and varies drastically depending on the reason and geography.4 Models can now be highly specific to particular bundle payment models. For example, we introduced highly performant models that specifically focus on identifying patients likely to surpass the maximum allowable amounts under a 90-day bundle for a particular procedure. Using precision models like these can be game changing in terms of providing new levers for avoiding unnecessary costs during a bundled payment period.
Empowering Shared Decision Making
Predictive analytics have the power to help in other decision-making areas as well. Imagine you are the patient and are presented with a medical decision, such as a knee replacement. You talk to your family and friends and use the internet for research, but what happens when you try to weed through complicated medical literature for evidence and when you meet with your doctor to discuss your options? Do you know which questions to ask, what evidence exists and what it means for someone like you, what outcomes you can expect, and what risks you will be taking on if you have the surgery? That’s where shared decision making and predictive models can come together to support evidence-based and more personalized decision making.
The concept of shared decision making has been around for a couple of decades. In that time, the principles of shared decision making have essentially remained the same and focus on clinicians engaging patients in medical decisions and centering those decisions around benefit, risk, and quality of life factors. The general consensus is that shared decision making leads to more engaged patients who feel more comfortable with their care plans and are more likely to stick to them. Shared decision making is also increasingly becoming part of reimbursement and quality initiatives.5 Typically, shared decision making includes different forms of education materials and clinician-patient conversations advising patients on the benefit and risk factors based on population-level or clinical trials data. What aggregate data from clinical studies does not reveal is what a particular patient’s likelihood of improvement is following surgery, given their very specific medical and functional characteristics and risk factors.
Applying similar precision technologies, shared decision making is also changing. For example, OM1 is collaborating with leaders in orthopedics at major medical centers to pilot new, patient-facing, shared decision-making tools that leverage AI to improve the doctor-patient conversation around treatments and outcomes with personalized and patient-centric information.
Need the right data to drive AI solutions
In order to generate useful information, AI models need to be developed from and applied to datasets that contain the key information that describe both the relevant characteristics of the patient and the outcomes of interest. With high performant models available today, events, such as complications, or costs can be accurately predicted based on standard medical information that can be automatically gleaned from the electronic medical record of a patient. However, in order to predict functional outcomes and benefit, such as for patient selection and shared decision making for joint replacement or spine surgery, it has been shown that baseline patient-reported outcomes and quality of life measures are critical information for predicting post-surgical outcomes. Practices seeking to use AI for those purposes need to collect patient information through standard instruments underlying these models, such as KOOS, HOOS and PROMIS, at least at baseline. Advanced, but cost-efficient systems, can now automatically collect follow-up data, and generate individual and practice level comparative outcomes benchmarks. Beyond the utility of the AI models for individual patients, the leverage from having valid outcomes metrics for orthopedic and spine procedures in value-based care negotiations is also becoming increasingly clear.
Conclusion
AI has many uses in healthcare, but advanced predictive modeling is the one gaining the earliest traction because of the opportunity to identify high risk patients and take action to optimize their success; avoid avoidable events and costs; and, engage patients in more meaningful shared decision making. AI-based solutions for hip, knee and spine procedures are becoming more common in community hospitals and practices as well as in academic centers. These tools are making orthopedic practice more measured, precise and pre-emptive and improving patient and financial outcomes.
1 Etkin C, Springer B. The American Joint Replacement Registry—the first 5 years Arthroplast Today. 2017 Jun; 3(2): 67–69. Published online 2017 Mar 14. doi: [10.1016/j.artd.2017.02.002]
2 Hogan CA, Sandoval MF, Uhler LM. Centers for Medicare & Medicaid Services' Comprehensive Care for Joint Replacement: The Present and Future for Orthopedic Surgeons. Orthopedics. 2017 Mar 1;40(2):77-80. doi: 10.3928/01477447-20170302-03.
3 Menendez ME, Schumacher CS, Ring D, et al. Does "6-Clicks" Day 1 Postoperative Mobility Score Predict Discharge Disposition After Total Hip and Knee Arthroplasties? J Arthroplasty. 2016 Sep;31(9):1916-20.
4 White RS, Sastow DL, Gaber-Baylis LK, Tangel V, Fisher AD, Turnbull ZA. Readmission Rates and Diagnoses Following Total Hip Replacement in Relation to Insurance Payer Status, Race and Ethnicity, and Income Status. J Racial Ethn Health Disparities. 5(6):1202-1214. doi: 10.1007/s40615-018-0467-0. Epub 2018 Feb 12.
5 Strategy 6I: Shared Decisionmaking. Content last reviewed October 2017. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/cahps/quality-improvement/improvement-guide/6-strategies-for-improving/communication/strategy6i-shared-decisionmaking.html